

Ian Brandon is a consultant for the Good Governance Institute, a management consultancy operating since 2009.
The GGI helps organisations scale up their operational and strategic maturity across the healthcare, charity, sports and arts sectors - with the NHS as its primary customer.
Qualsys spoke to Ian to learn about:
- How NHS trusts can embed lasting quality improvement
- What 'good governance' really means for the future
- The ingredients of world class healthcare quality

Qualsys: How does the Good Governance Institute approach an organisation like the NHS?
Ian: Well our primary focus, as you might expect, is governance.
But governance is sometimes misunderstood. It's not just about getting systems and processes in place. We interpret it to include things like stewardship and leadership as well. Stewardship is a huge part of governance.
Fundamentally that means looking after an organisation and making it a better place before the next leaders come in to steward.
We perform diagnostic and improvement initiatives using matrices which focus primarily on two things:
1) how things work, and
2) how well developed an organisation is.
We score each NHS trust from 0-5 in maturity: 0 being disconnected or non-existent governance, and 5 demonstrating a fully integrated, embedded, cultural approach to governance.
If we look at something like information, intelligence and reporting, we can see the difference between a mature trust and an immature one.
For example, in a mature trust, reporting would be in real-time but would also focus on the strategic priorities of the organisation.
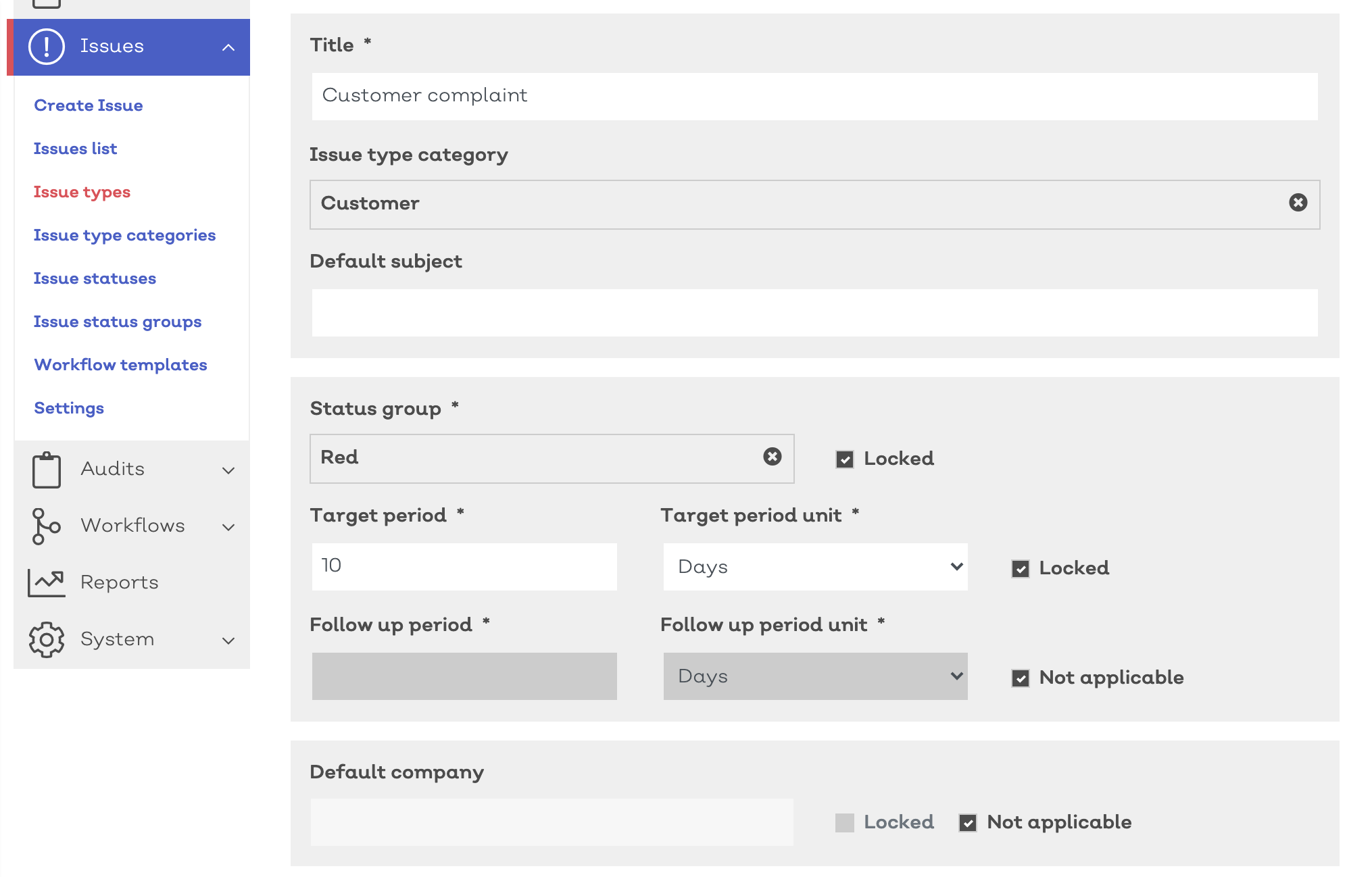
A good performance dashboard should include things like statistical process control (SPC) charts, RAG ratings and trend lines, with real time reporting. But the key objective is to report and use data in a triangulated way, with a focus on the organisation's strategic objectives.
So one trust had an issue with pressure ulcers. They compared occurrence data with things like staffing data and handover data, to look for a pattern. But it's also important to look for patterns that don't make sense or don't correlate - then you can look for deeper root causes, like leadership.
That's a bit more dynamic and bit more focused than just looking at numbers.
Stewardship is a huge part of governance. Fundamentally that means looking after an organisation and making it a better place before the next leaders come in to steward.
Qualsys: Is this digitisation of quality and deeper focus on data inevitable for healthcare?
Ian: Absolutely. It's something already occurring at board level. Less mature boards are looking at their data in a very linear fashion. They're looking at numbers and workforce-related dashboards in isolation, without painting a picture of how the organisation is really working.
Moving to integrated reporting and looking at the cross-themes and the discussions they create really gets boards and committees to think about why the data is saying what it is.
That pushes management to triangulate what's going on and what the actions might be in relation to improvement. Or it might show good practice that could be replicated elsewhere.

Qualsys: What do you think is the main mistake trusts make that stops them moving up the scale from 0 to 5?
Ian: The biggies are normally twofold.
One is always leadership. If you haven't got a good leadership team that understands where their team is and how to motivate and focus, that really hampers improvements. If you don't have buy-in for improvement, you'll get nowhere.
Moving to integrated reporting and looking at the cross-themes and the discussions they create really gets boards and committees to think about why the data is saying what it is.
In good trusts that we hear about like Salford, Frimley, Western Sussex among others, there's that trend of leadership teams celebrating their successes but always wanting to improve.
A lot of companies focus on continuous improvement, but only from a systematic perspective. So they're putting together quality improvement programmes without thinking about making sure it's embedded in the culture so people want to continually improve.
The other issue we see is organisational memory: reinventing the wheel a lot. That means things that have worked before getting dropped off, and things that haven't worked before getting rehashed and reused. That sometimes happens when there's a new executive team or a new board. There's a pressure to redo strategies and plans, but actually if there had been a better handover from old leadership it would have been easier to get an organisation to continue on its journey, rather than having to restart and stop/start.
That's a big frustration for a lot of the staff we work with.

The Seattle-based Virginia Mason Institute has teamed up with the
NHS since 2016 to introduce lean quality management techniques
Read our article: 'Capita's quality auditor talks mental health and the NHS'
Qualsys: What would you say is the main way to start implementing a quality culture?
Ian: It starts with leadership and creating a culture that's open and transparent - that 'everyone's in it together' type of mantra.
Leaders always need that ability to bring people with them while making them feel that they're also part of the team themselves, rather than being superheroes.
Having those distant leaders was the old-fashioned way. Now it's very much everyone working to the same message, and leaders supporting and opening doors and barriers to allow things to happen. That openness and transparency lets you move onto how you can make the improvements you need to make.
One of the things that's going to be interesting in the new ways of working after COVID is: with organisations having to be more virtual, how do you foster that organisational creativity?
At the GGI we've been thinking what kind of technological solutions will help virtual ways of working, to enable staff to be creative together in ways that's not just another meeting. When you're working from home, you just don't have the ability to speak to people as much, unlike the corridor and office conversations we're used to when we work in the same place.
That dynamic of acceptability and involvement needs to be replicated in the virtual world - we just need to find the best way to do it.
Qualsys: Could you share a good news story you've seen from a NHS trust?
Ian: Brighton's the one to talk about.
Brighton was a trust who had to turn things around. They had an inadequate CQC rating and we started working with them about 2 years ago to change their governance structure, to make quality a clear stream of work that reached all the way down the organisation.
We helped them build proper integrated reporting, and brought a new leadership team in.
Slowly but surely, they've turned things around and they're now rated 'good'. It's taken them a while.
The key was putting the framework in place for continuous improvement, and making sure their leadership could drive it. That's what happened there.

The Brighton and Sussex University Hospitals NHS Trust turned
things around with a thorough governance and continuous improvement plan
Qualsys: What future trends can you foresee for quality and governance in healthcare?
Ian: The GGI has been thinking a lot about this.
In the short term, it will probably take 6-12 months for a 'new normal' to develop after the lockdown. There has to be good governance in place for making those plans to start going back to dealing with targets, dealing with quality, with regulations, strategic thinking, digital transformation and so on.
What we're saying in our bulletins is that businesses and trusts need to make sure those conversations are allowed to happen, and those plans are being worked on and met.
The key was putting the framework in place for continuous improvement, and making sure their leadership could drive it. That's what happened for Brighton.
What the outcome of that will look like in a good organisation is that the trust strategy will be looked at and amended. What they'll find is a lot of the plans in a strategy from 2-3 years ago will have been accelerated by COVID: digital transformation being one of them, as well as how a trust works with the environment, meets new regulatory pressures, deals with finance, and so on.
The key thing will be looking at what has been accelerated and what needs focusing on for the future. That strategy needs to be the focus of the organisation, while thinking strategically, rather than just operationally.
The other trend will be a change in how system-working governance will look. At the moment there's no legislation for ICSs or ICPs, it's very guidance-based. Part of the work we do with organisations is helping them meet that system-based working.
A lot of the plans in a trust strategy from 2-3 years ago will have been accelerated by COVID: digital transformation being one of them.
Organisations have reacted in different ways to COVID: some have been very isolated, some have looked at the whole system a lot better. So looking at the governance requirements and weighing up how to balance sovereignty of an organisation with working within a system is going to be one of the key areas that needs to be thought about.
How they work to ensure that that system integration for the overall improvement of quality in health and social care really works.
Qualsys: What do you think the long-term impact of digital quality management tools will be?
Ian: There are two dimensions to this: improvement and risk.
Being able to look at patient records across different areas in a standardised way is going to be massive. We've seen that work in Finland. It's about holding each other to account and understanding how the entire system works rather than focusing on individual providers.
At the same time, all that data needs to be controlled and shared safely and properly. We in the UK value our liberties and protections more than other countries that work in a more systematic way - so we're going to have to make that trade-off between what protections we're willing to sacrifice versus making our healthcare a more integrated system. And technology is going to be a big part of that.
Governance is ultimately about stewardship and passing on an organisation in a better state than it was in before. That's going to be a huge part of how leaders need to start thinking going forward. If that's a principle that becomes more mainstream in thinking about how leaders work, we'll be in a better place.

![]()
Keep learning
Follow our customer NHS Huddersfield Pharmacy Specials on their quality journey by watching our case study video:



Share your thoughts on this article